
By Shaina Cole | Contributing Writer, Rocky Mountain Voice
Colorado’s state budget is larger than it used to be. That much isn’t disputed.
What has changed over the last twenty years is where that growth landed.
The Common Sense Institute’s “Colorado Budget: Then and Now” (December 2025) Colorado’s state budget has grown faster than population and inflation since the mid-2000s. The shift wasn’t sudden. It accumulated, year by year, across multiple budgets and multiple administrations.
The increase shows up clearly in the numbers.
In the mid-2000s, state spending worked out to a little under $5,600 per person once population and inflation were accounted for. It didn’t stay there. Year by year, the number crept higher. It now sits above $7,300. The increase didn’t happen overnight. It crept in, budget by budget.
The biggest increases didn’t show up right away. Those came later, overlapping with growing warnings about the budget getting tighter.
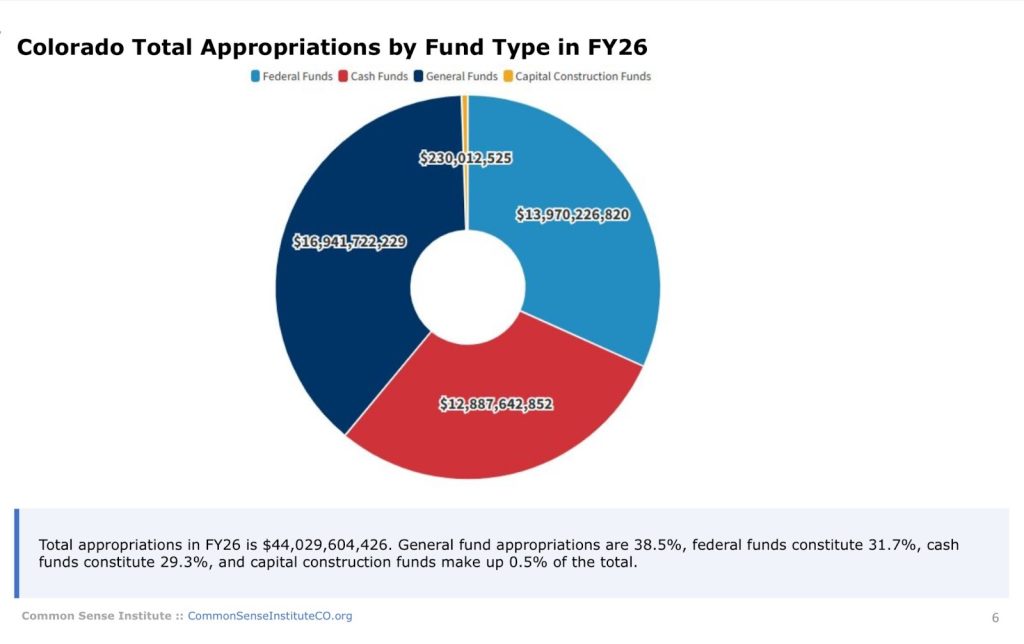
The 2026 budget cycle dragged on. Lawmakers debated it for months. In the end, what reached Governor Polis for 2026 totaled just under $44 billion.
The size draws headlines. Where the money ends up matters more.
One department now dominates the budget
The shift shows up most clearly in one place.
The Department of Health Care Policy and Financing — the agency that runs Medicaid and related programs — now occupies a central role in Colorado’s budget.
Roughly two decades ago, the department handled a little more than $3 billion. Its budget has since climbed past $18 billion.
That change alone reshaped how state dollars are allocated. Over the same period, health care’s share of the overall budget grew from roughly one-fifth to nearly half, according to the Common Sense Institute’s analysis.
And the trend hasn’t slowed.
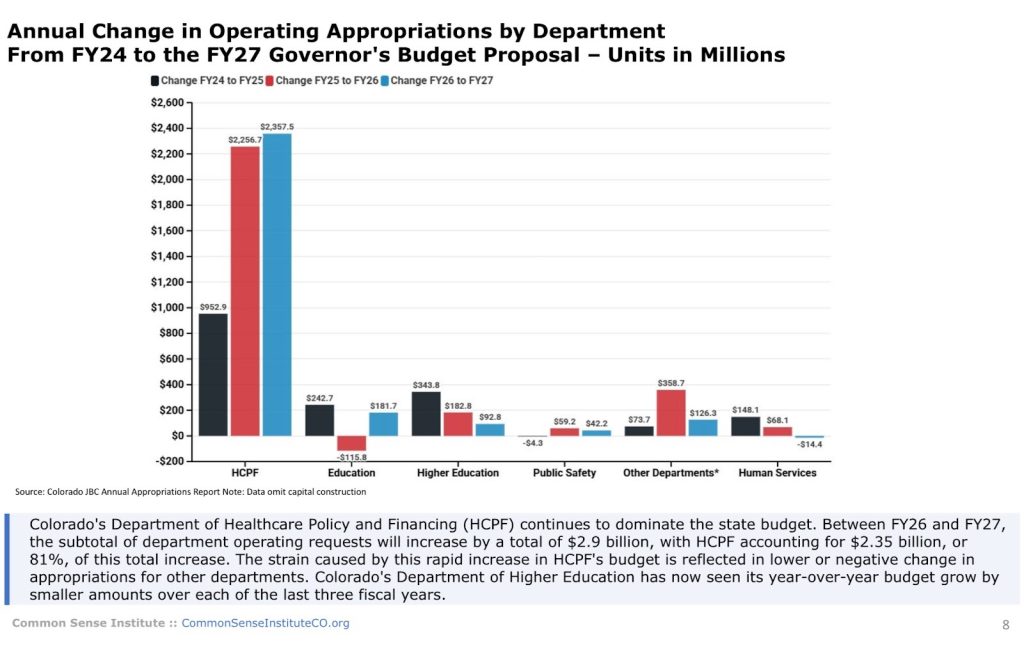
In the governor’s proposed fiscal year 2027 budget, health care accounts for 81% of net operating budget growth and about 70% of projected General Fund growth from fiscal year 2026. Even in years when overall appropriation growth eases, health care continues to absorb most new dollars.
Why the floor keeps rising
This didn’t happen in a single year. The baseline itself moved.
Medicaid enrollment surged during the pandemic under federal continuous-coverage rules. When those rules ended, enrollment declined — but not back to where it started. The state is now budgeting from a higher starting point than it did before COVID.
Medicaid’s cost structure has also shifted over time. Seniors and people with disabilities account for a relatively small share of total enrollment, yet they represent a far larger share of spending. The result is higher per-person costs. Medical price pressures add to it, with health care expenses outpacing inflation in many years.
Federal matching funds amplify those changes. When Colorado increases Medicaid spending, federal dollars follow. The Common Sense Institute notes that federal funds now make up nearly one-third of the state budget. Health care programs account for a significant share of those federal dollars, and policy expansions can carry long-term fiscal obligations.
Emergency rooms, migration, and coverage expansions
Emergency care plays a role.
Under federal law, full Medicaid coverage is limited by immigration status. Emergency Medicaid follows a separate framework. States must still ensure access to qualifying emergency care.
Emergency Medicaid provides reimbursement for some qualifying emergency care, though hospitals continue to report high levels of uncompensated care from uninsured emergency department visits.
During the Biden administration, Colorado experienced a significant influx of migrants—many arriving without health insurance. Hospitals along the Front Range have reported higher emergency room use by uninsured patients.
The CSI report does not separate health care costs by immigration status… but Emergency Medicaid flows through the same department now driving overall budget growth.
Colorado has also expanded state-funded coverage beyond emergency care. The Cover All Coloradans law extended full Medicaid and CHP+ benefits to low-income children and pregnant people regardless of immigration status. Separately, the OmniSalud program offers state-funded subsidies for private insurance to people excluded from the federal marketplace.
At current enrollment levels, OmniSalud alone costs the state roughly $75 to $80 million per year — about $6,600 per enrollee annually.
Emergency rooms add another layer. Not every visit is a true emergency. Emergency departments are frequently the default option for routine or non-urgent care when patients lack access to primary care. Because emergency care is one of the most expensive settings in the health system, higher utilization — even for non-emergencies — pushes costs higher across the system.
At the same time, federal officials have opened investigations into aspects of Colorado’s migrant response, placing additional scrutiny on how health care and related services are being funded and administered.
The quieter effects on people who already have insurance
These shifts don’t stop at public programs.
Hospitals don’t get to turn people away. That includes patients without insurance. When payments don’t cover the cost of care, those losses add up over time.
Hospitals absorb a significant share of uncompensated care. The remainder shows up in higher prices negotiated with private insurers.
As public coverage and subsidized insurance expand, demand for care rises. Provider networks — already strained by workforce shortages — feel the pressure. For people with private insurance, that can mean longer waits for appointments, narrower networks, and higher premiums, deductibles, and co-pays, even if they never enroll in public coverage themselves.
Premium growth affects who stays insured and who doesn’t. A Kaiser Family Foundation survey found rising costs prompt many people to consider dropping coverage or switching plans. Roughly one in four respondents said they would be very likely to go without insurance. Long-term health policy research by the National Institutes of Health shows a similar pattern—linking even modest premium increases to measurable growth in the uninsured population.
Locked-in costs, limited flexibility
Governor Polis has warned that budget conditions are tightening and has proposed reductions or slower growth in some areas of state government. Health care programs created or expanded through legislation tend to be treated differently.
Over several of the last legislative sessions, Colorado expanded Medicaid eligibility and benefits. Lawmakers also lengthened postpartum and continuous coverage periods and added more behavioral and mental health services. Provider reimbursement rates were increased. New administrative layers followed. Together, those changes created ongoing obligations that must be funded year after year.
That reality leaves lawmakers with fewer levers to pull when revenues flatten.
A long-term tradeoff
The Common Sense Institute report doesn’t argue that health care spending is unnecessary. However, it shows how central it has become to Colorado’s budget.
Nearly half of state appropriations now flow to health care, and in recent years it has grown faster than any other major area of the budget.