
By Shaina Cole | Contributing Writer, Rocky Mountain Voice
An unvaccinated traveler touched down at Denver International Airport after eleven hours in the air — measles already working through the bloodstream, picked up in the U.S. before the trip out. One night in a Denver hotel. Back to the airport the next morning and onto a domestic flight home.
By the time Colorado public health officials finished tracing what followed, ten state residents had confirmed measles. Nine exposed during that single pass through DIA — on the flight, in the terminal, at a gate. One more from a household contact downstream.
Four of the nine secondary cases — including three passengers on the international flight — had received both recommended doses of the MMR vaccine. Measles lingers airborne for two hours after an infected person leaves a room — full vaccination reduces the risk dramatically, but not to zero in conditions like those. The CDC published the event as a formal case study.
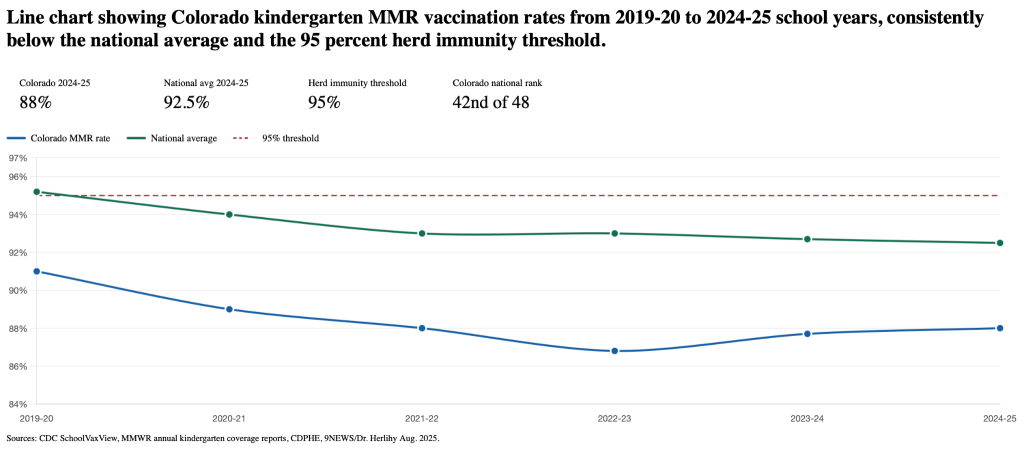
Eighty-eight percent. That’s Colorado’s kindergarten MMR vaccination rate going into 2025 — 42nd in the country, below the 92.5 percent national average. The threshold for stopping measles in a community is 95. Three points doesn’t sound like much until you run it out over five years. Roughly 9,000 fewer vaccinated kindergartners entering Colorado classrooms each year than there used to be.
The outbreak didn’t come from a policy decision or a crossing point. It came the way every major U.S. measles outbreak has come since 2000 — a virus looking for people who weren’t covered, in a place where enough of them lived close enough together to keep it moving.
Ask a Colorado conservative what caused it and you’d hear about open borders. Ask a progressive and you’d hear about Kennedy and the administration’s posture on vaccines. Both answers had something behind them. What neither had was the whole thing.
Where this actually started
In 1998, a British physician named Andrew Wakefield published a paper in The Lancet suggesting the MMR vaccine caused autism. The data was fabricated. It took twelve years for the journal to retract it and for Wakefield to lose his medical license. What it didn’t take twelve years to do was spread.
By the mid-2000s the claim was on daytime television. Jenny McCarthy appeared on Oprah attributing her son’s autism to the MMR shot. Jim Carrey amplified it. In 2008, the two organized a Washington rally called Green Our Vaccines, and Kennedy spoke there — not yet a federal official, but already a visible participant in a movement a decade in the building. He had been writing since at least 2005 about what he described as suppressed evidence linking vaccine preservatives to neurological damage.
What followed in specific communities is documented in CDC records. MMR coverage in Minnesota’s Somali-American population exceeded 90 percent before 2008, then fell to 42 percent by 2017 after anti-vaccine advocates — Wakefield among them, who visited Minneapolis personally — targeted parents already alarmed by elevated autism diagnoses among their children.
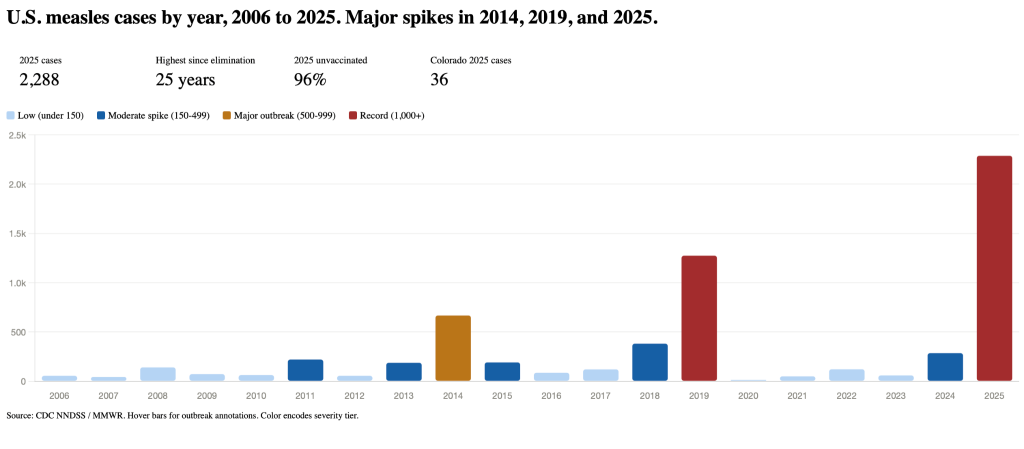
Outbreaks followed in 2011 and 2017, both linked directly by the CDC to that decline. An underimmunized Amish community in Ohio produced 667 cases in 2014. Orthodox Jewish neighborhoods in New York drove most of the 1,274 cases reported nationwide in 2019 — the previous post-elimination record — after unvaccinated travelers returned from Israel.
What the border argument gets right
The claim that inadequately vetted immigration contributes to measles importation is not a political talking point. CDC’s own Morbidity and Mortality Weekly Report confirms it, more than once.
Venezuela’s childhood measles vaccination rate was 68 percent in 2021. Three years later, in Chicago, 57 cases showed up at a migrant shelter.
It wasn’t the first time the pattern had appeared.
A 2016 outbreak at an immigration detention facility in Arizona made it into CDC’s published record.
In 2021, 47 of the 49 measles cases reported nationwide that year occurred among Afghan evacuees during Operation Allies Welcome. Mass vaccination stopped the spread.
Those events belong in any complete account of how measles enters the country.
What last year’s data won’t support is making them the central explanation. Of 2,288 confirmed U.S. cases in 2025 — the highest annual count in the 25 years since elimination — 25 involved international visitors of any kind. Roughly one percent. The outbreak ran approximately 90 percent on local transmission, ignited in Gaines County, Texas, in a community that state and federal health data had flagged as severely undervaccinated long before any policy debate about the border.
The community the data had already flagged
Gaines County is home to a significant population of Old Colony Mennonites. Mennonite Church USA has stated explicitly that its doctrine contains no theological basis for vaccine exemptions. The Old Colony community homeschools most children and enrolls others in private schools that fall outside state immunization reporting systems. Their actual vaccination rates are largely invisible to official data.
The county’s reported kindergarten exemption rate approached 20 percent in 2025. The Texas state average was under 4. CDC and state analyses had consistently placed Gaines County at the bottom of Texas MMR coverage — and because most Mennonite children are never counted, the true rate is likely lower than any figure on record.
Two children died. Both unvaccinated.
The CDC estimates 1 to 3 deaths per 1,000 measles cases in the U.S.
Kennedy, vitamin A, and what the science says
At the administration’s first cabinet meeting in February 2025, Kennedy described measles outbreaks as “not unusual.” He misstated the death count and incorrectly characterized why patients were hospitalized. Texas health officials corrected both publicly.
His Fox News op-ed described vaccination as “a personal” decision — language that departed from how HHS secretaries of both parties had responded to prior surges. In 2019, Secretary Alex Azar issued a direct pro-vaccine statement.
President Trump, asked that year what parents should do, was unambiguous. He stated, “They have to get the shots.”
What drove the national conversation wasn’t the cabinet meeting. It was Kennedy’s public promotion of vitamin A supplements and cod liver oil while the outbreak was still expanding.
The record on vitamin A is more nuanced than the coverage suggested. WHO and CDC do recommend physician-supervised vitamin A supplementation for children with active measles — studies show it can reduce mortality in children under two.
The problem in Texas wasn’t the recommendation. It was the absence of medical supervision. The New England Journal of Medicine documented vitamin A toxicity cases in West Texas linked to excessive, unsupervised intake driven by public misinformation.
Cod liver oil is a separate matter. The American Academy of Pediatrics states it has no evidence base for measles and poses its own toxicity risks in excess. CDC recommends consulting a physician before any supplementation.
In April 2025, Kennedy told CBS News, “The federal government’s position, my position, is that people should get the measles vaccine.” It was the first time he had said it publicly since taking office in January.
His argument has not been that vaccines should be abandoned. It has been that the existing schedule moves too fast, that safety testing is insufficient, and that parents deserve the right to make informed decisions.
The ingredient that drove Kennedy’s earliest concerns was thimerosal, a preservative used in some vaccines. It hasn’t been in routine childhood immunizations since the early 2000s. Autism rates went up after its removal, not down — the opposite direction causation would require.
The more recent focus has shifted to aluminum adjuvants. A 2025 Danish study followed over a million children looking for exactly that connection. It didn’t find one. The broader body of research — studies spanning hundreds of thousands of children across multiple countries — has been consistent on the MMR vaccine specifically. No causal link to autism.
Research into schedule timing, adjuvant effects in specific subpopulations, and individual risk factors is ongoing, and the mainstream scientific community takes those questions seriously.
The vaccination rate decline fueling last year’s outbreak preceded Kennedy’s confirmation by years.
The context that keeps getting cut
Canada lost its measles elimination status in late 2025 — falling vaccination rates, undervaccinated close-knit communities including Mennonites, importation events feeding into gaps that had been growing for years. Different country, different government, same outcome.
The United Kingdom lost elimination status in 2018. Regained it in 2021. Lost it again in January 2026 — alongside five other European countries, based on 2024 data. The World Health Organization reported global measles vaccine coverage dropped to 81 percent in 2021 — the lowest since 2008.
The resurgence is not an American political story wearing a public health costume. The politics arrived later, layered on top of something developing across most of the Western world since a single fraudulent paper landed in a British medical journal.
And it isn’t over. As of mid-April 2026, the United States has confirmed 1,748 measles cases so far — 94 percent tied to outbreaks that began in 2025. South Carolina has become the new epicenter.
Its outbreak started in October in Spartanburg County, centered in a Ukrainian and Eastern European immigrant community where some schools reported MMR coverage as low as 21 percent. It reached 997 cases before showing signs of slowing in late March — surpassing the Texas outbreak to become the largest single outbreak since elimination.
Utah is now recording its own surge with more than 600 cases.
Colorado is again among the affected states, with 16 confirmed measles cases in 2026.
Both sides of this latest debate have had years to tell the full story. One found a villain in a cabinet secretary. The other found one at the border. The virus, for its part, doesn’t follow a narrative. It follows a gap. And in Colorado, that gap is still open.
Editor’s note: This story was updated on April 23, 2026 to add the current Colorado case count and CDC data on measles mortality. As of April 15, 2026, Colorado has confirmed 16 measles cases in 2026, concentrated in five counties.