

By Jen Schumann | Rocky Mountain Voice
Just after midnight, an 18-year-old Colorado woman—identified here as “Clarity” to protect her identity—went to the ER, hoping the pain was only a severe case of gastritis.
She’s a recent high-school graduate now working for a Colorado nonprofit and was granted anonymity by RMV.
When Clarity was finally told she could leave, someone brought over an iPad and said she needed to finish a few discharge questions before going home.
On the screen was Colorado’s Patients’ Right to Know Act Service Availability Form—pages of items about gender-affirming care, abortion services and end-of-life options.
“She was yelling at us over Zoom, saying, ‘Do you understand that you have access to these services and you’re knowingly denying them?’” Clarity recalled. “My mom said, ‘We don’t want to answer these questions.’ The lady said, ‘I can’t let you leave until you answer these questions.’ It was one in the morning—we just wanted to go home.”
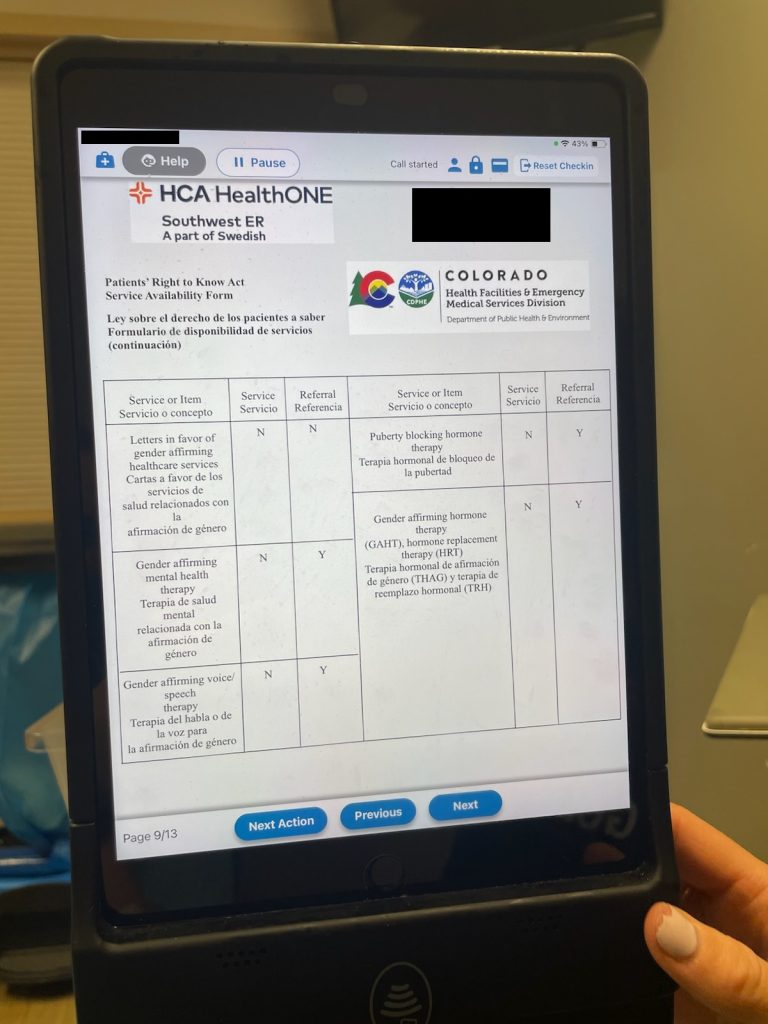
The hospital’s discharge iPad displaying Colorado’s Patients’ Right to Know Act form, page 9 of 13.
The discharge questionnaire turned into what felt like a standoff. The staffer’s words made the encounter unmistakably bureaucratic.
Her memory of that night is sharp, shaped less by pain than by the feeling of being processed. “It was honestly very violating—not just of my medical privacy but of my religious practices,” Clarity said.
The experience drove her to research why an emergency room visit for abdominal issues included a forced—and repeated—interaction about gender ideology. What Clarity found left her disgusted—not only by how gender ideology shows up in patient intake, but by how it has been institutionalized at the hospital level.
“I think that every Coloradan should know that you can’t afford to be asleep anymore,” Clarity said. “People are falling victim to this every day—people who aren’t grounded in their beliefs or sure of what’s right and wrong. It’s very, very wrong. It’s not what it’s being presented to be.”
To her, what happened wasn’t just a healthcare visit gone wrong but evidence of a law that turns medical visits into ideological compliance exercises.
A system built on deadlines and data
The process traces back to HB23-1218, the Patients’ Right to Know Act. Lawmakers and CDPHE pitched it in 2023 as a consumer protection measure meant to give patients “clear and simple” information about services. But once the stakeholder meetings began, the focus shifted from transparency to compliance.
In the first session on September 26, 2023, CDPHE policy manager Alexandra Hawes described HB23-1218 as “a consumer protection law… really about a patient’s consumer rights.” By October 24, policy advisor Ash Jackson was describing something far more expansive: “My guess is probably 700 individual points of data for every health facility… and about 170 health facilities. That’s a lot of data to display.” He said the final product would be “a searchable website—a few clicks for them to find a facility that does provide it.”
Those data points aren’t limited to general services. They drill down into some of the most controversial areas of medicine.
The lists covered gender-affirming procedures like puberty blockers, hormone therapy, bilateral mastectomies, vaginoplasty and phalloplasty. “It’s wrong because you’re perpetuating social contagions in youth and planting ideas in their minds that turn normal adolescent discomfort into something else,” Clarity said. “You’re telling them they’re transgender—and that’s inherently harmful. It leads to sex changes; it leads to suicide; it leads to extreme mental-health problems that go far beyond gender dysphoria.”
The form also includes info about reproductive care such as contraception, sterilization, in-vitro fertilization and abortion, along with miscarriage and ectopic pregnancy management. End-of-life categories captured medical aid in dying, hospice and palliative care, withdrawal of nutrition and honoring advance directives.
“The bill presented reproductive care, abortion, gender-affirming care and end-of-life care—all as good things,” Clarity said. “To me, that’s a direct attack on life and on children, on the youth of our generation.”
The form went public in June 2024, facilities had 60 days to submit, and by Oct. 1, 2024 every facility was required to hand the form to patients at scheduling and again with HIPAA intake.
Hospitals must keep proof that patients receive it, while CDPHE collects each facility’s completed form and publishes it online so the public can see which services are available, restricted or denied.
CDPHE has since launched the Health Facility Service Availability portal, where the completed forms for every licensed hospital and clinic can now be viewed publicly. Facilities that don’t comply can be fined up to $1,000 a day.
Provider pushback meets compliance at the table
As the process unfolded, providers warned that conscience protections and constitutional limits were being pushed aside. Faith-based hospitals objected that long-standing conscience policies were now labeled “nonmedical denials,” erasing their legitimacy.
That conscience-based objection isn’t theoretical, says Clarity, “If I wasn’t so grounded in my beliefs, it would’ve been easy to cave. They just kept pushing me to accept something I never asked for.”
By April 2024, the debates had escalated to explicit constitutional warnings. Even supporters warned the rule could overstep constitutional limits. “We remain very concerned and opposed to the inclusion of the links at the very end of the companion document… it could create a potential court challenge for this entire law as compelled speech,” said Philip Shimel of Cobalt Advocates.
Heather Shumaker of the National Women’s Law Center agreed, pointing to the Supreme Court’s NIFLA v. Becerra ruling, which struck down mandatory notices on First Amendment grounds.
For Clarity, the legal arguments echoed what she had already sensed about the system’s reach. “It’s not constitutional and it’s not aligned with free enterprise,” she said. “It’s pinpointing each hospital’s ideological stance. Why do they need that? Hospitals are private businesses. Why don’t we have data points on tattoo parlors or bars? It just smells very funny.”
An uncommon researcher at 18
Most teenagers don’t spend evenings watching rulemaking hearings. After her hospital visit, she pulled up the department’s public Google Drive and watched long sessions, taking notes on end-of-life, LGBTQ and reproductive debates. “I think I watched about six,” she said. “I took notes because I wanted to understand how they were justifying this.”
The more she watched—she realized—authority doesn’t equate to wisdom. “We put people on pedestals because of their titles. But they’re just regular people—who don’t always know what they’re doing,” Clarity said. “The compassion narrative in those meetings was alarming—it felt more like manipulation than mercy.”
What struck her most wasn’t just what she heard in those meetings—it was how few people outside of them seemed to notice. “There was not one media story on 1218,” Clarity said. “No objection in the public square—reminds me of that quote from Nazi Germany—the one about the pastor who didn’t care when they came for others until they came for him.”
But Clarity reflected, “It feels that way now, but there’s still hope. If it can swing this far one way, it can swing back.”
The bigger stakes
What happened that night changed how she thinks about care and authority. “The only reason I didn’t break was because of my faith,” she said. “I just kept reminding myself this wasn’t care, it was compliance.”
“It violates freedom of religion,” she said. “Beyond that, it violates your ability to believe something and not practice it. We’re rubber-stamping everybody as compliant, even when people have genuine ideological objections.”
“They redo the stakeholder process every two years to add new rules.” Clarity added, “And people should know they can speak up if they think this is wrong or unconstitutional.”
Clarity left the hospital shaken but steady, convinced that faith—not policy—had kept her grounded. The law may define care in codes and data points, but she still sees something bigger at stake: conscience and the right to say no.